An interesting presentation of Nephritic- nephrotic syndrome with Mitral valve stenosis
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient-centered online learning portfolio.
Here is a case i have seen:
45 year man presented to our opd with the complains of Dyspnea since 1 week
Abdominal distension since 5 days
Swelling of bilateral upper limbs, neck and face since 5 days
Reduced urine output since 5 days
Reddish colored urine since 3 days
Slurred speech since 3 days
He worked as a Farmer for 25 years and worked as a watchman until 1.5 years back since when he has been at home on bedrest. He got married to a coolie and has adopted a daughter. He got diagnosed to be a hypertensive and diabetic 15 years back and has been on oral medications since then but hasn't been taking any of his medications since the last 3 months. He was an occasional alcohol drinker the last 25 years.
15 years back he lost his right little finger while he was working in his paddy field when a tractor went over his little finger.

His amputated right little finger
He used to work as a watchman until 1.5 years back until one day when a. gate fell on his right lower limb after which he attained fracture of his right hip for which he got operated at Gandhi hospital. He walked with the help of a stand for half an year. Since the last 1 year he has been completely on bedrest and says he started consuming around 90 to 180 ml of whisky everyday and he says that he often felt sad as he couldn't perform his day to day activites and was dependent on others. His last alcohol intake was 1 week back.
He also tells he has taken a good amount of painkillers for pain relief. He has been regularly paying visits to local hospitals for pain relief where he was given pills that reduced his pain effectively.
Since 1 week he has been having dyspnea on and off since a week, abdominal distension since 5 days, swelling of both upper limb & lower limbs, neck, facial puffiness since 5 days
Reduced urine output since 5 days
Red coloured urine since 3 days
His dyspnea was sudden in onset and gradually progressive though on the day of presentation it wasn't associated with any cough, palpitations, orthopnea, PND, hemoptysis. Over the next 5 days he observed that he abdomen was distended and he even developed swelling of both the upper limbs and lower limbs over the next 4 days.
He even developed facial puffiness since 3 days.
He also tells that his urine output has reduced since 5 days.
Red colored urine since 3 days.
He also gives a 5 years history of dyspnea on exertion on and off since 5 years and often would have palpitations on & off which the patient described as 'Gunde dada'.
On presentation , he was obese, he was brought to us on a stretcher. The first thing we noticed was that he was tachypneic with a respiratory rate of 26 cpm.
He had clubbing ( Parrot beak type)

He had facial puffiness along with swelling of the neck, bilateral upper limbs and lower limbs.


He was already on Foley's catheter and we noticed high coloured urine in his urobag

Bp was 70 at presentation
PR at 96 bpm
Temp - 98.6 F
Spo2 - 96 %
CVS - S1, S2 +
Lungs - Left, right IMA, IAA reduced breath sounds
Abdomen - Non tender on palpation
Bowel sounds were heard
He was conscious, coherent and cooperative
There was no Cranial nerve abnormality
Power : Right Left
Upper limb 4+/5 4+/5
Lower limb 0/5 2/5
Reflexes - biceps was present bilaterally, though couldn't elicit other upper limb reflexes because of the edema
All of his lower limb reflexes were absent
Plantar reflex was mute bilaterally
The patient was started on fluid resuscitation and his BP was brought upto 150/80mmhg
10 % calcium gluconate was given for his hypocalemia
along with Potassium deficit correction






Usg abdomen:

2d echo:
HOCKEY STICK SIGN - SUGGESTIVE OF MITRAL STENOSIS

Mitral valve surprisingly measures 3.7 with such a moderate Mitral valve stenosis

HRCT Thorax:


Bleeding time-2 mins
Clotting time-5 mins
Prothrombin time- 19 secsC- reactive protein- negative
Serology for HCV, HIV, HBSag was done which was found out to be negative
His Problems were :
40 year old man, hypertensive and diabetic since 15 years
Paraplegic since 1.5 years presented with
Dyspnea since 1 week
Generalized anasarca since 6 days
Hematuria since 5 days
Slurred speech since 3 days
Problems to be dealt with :
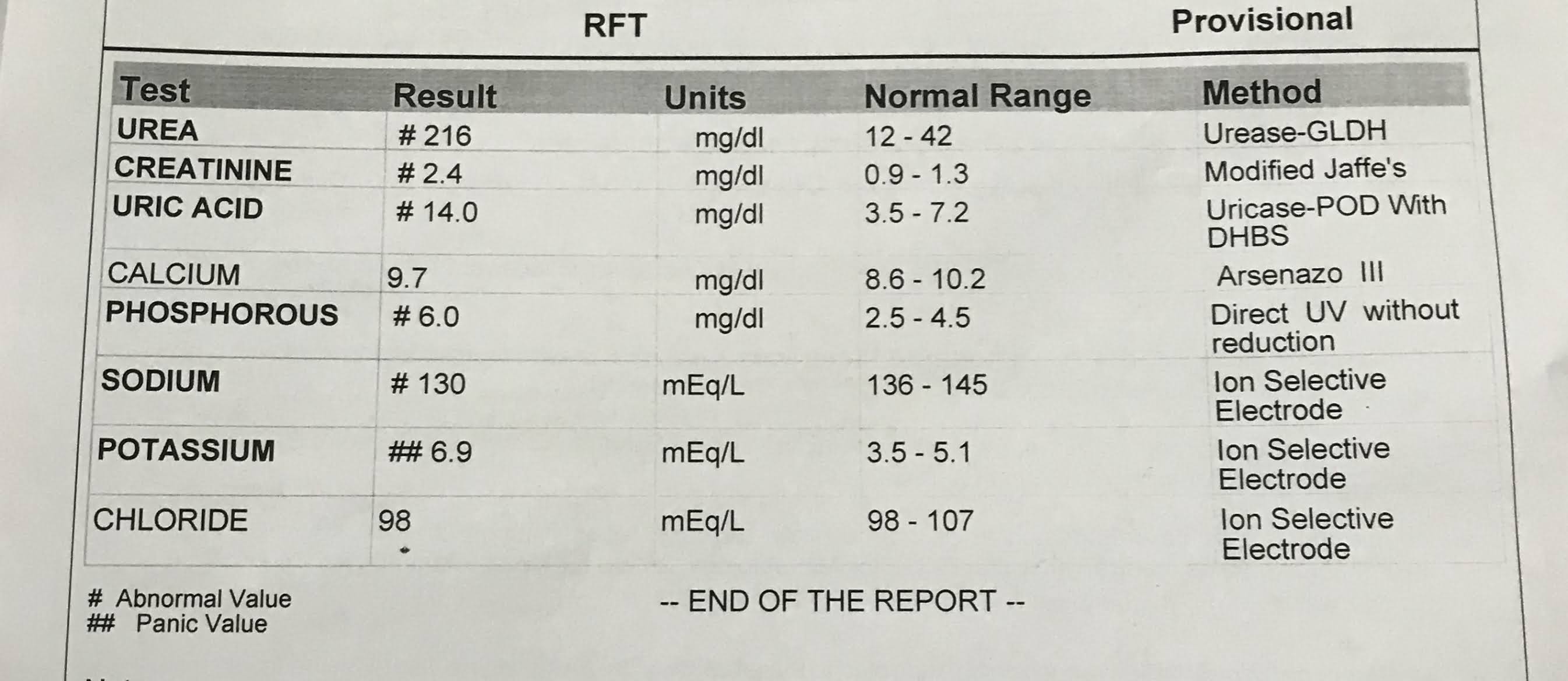
Metabolic acidosis
Hypoalbuminaemia
Albuminuria
Hematuria
Hypocalcemia
With deranged coagulation profile
B/L pleural effusion Rt>Lt
A Provisional diagnosis of - Nephritic Nephrotic syndrome with eGFR -54 ml/min/1.73m2
HFPEF
PAH with Mitral Stenosis
Hypertension and DM TYPE 2 since 15 years
Right eye cataract since 15 years
Monoplegic since 1.5 years
B/L Pleural Effusion ( RT > LT)
The patient was started on fluid resuscitation and his BP was brought upto 150/80mmhg
10 % calcium gluconate was given for his hypocalemia
along with Potassium deficit correction
For Hypoalbuminaemia we had a debate whether or not to start him on Albumin infusion as his serum albumin was as low as 0.68, we decided to consider going ahead with oral albumin supplementation rather instead of the cost effective albumin infusion which would be anyway lost into his urine in no time.
His Presention made us come to a provisional diagnosis of
Nephritic - Nephrotic syndrome probably following an infective etiology with such an acute presentation
Hypocalcemia due to hypoalbuminaemia
- Day 2:







- DAY 3
S- Patient was complaining of increase of facial puffiness
The patient was even complaining of non productive cough
O - His Urine Input output was - 1700/1000ml
PR - 103 bpm
Bp 130/80
Temp - 98.4
Grbs -120
Lungs- reduced breath sounds in B/L IAA
Inspiratory crepts in Right IAA
Abdomen - diffuse tenderness
He passed his stool 2 days back
Bowel sounds +
Cvs - S1,S2
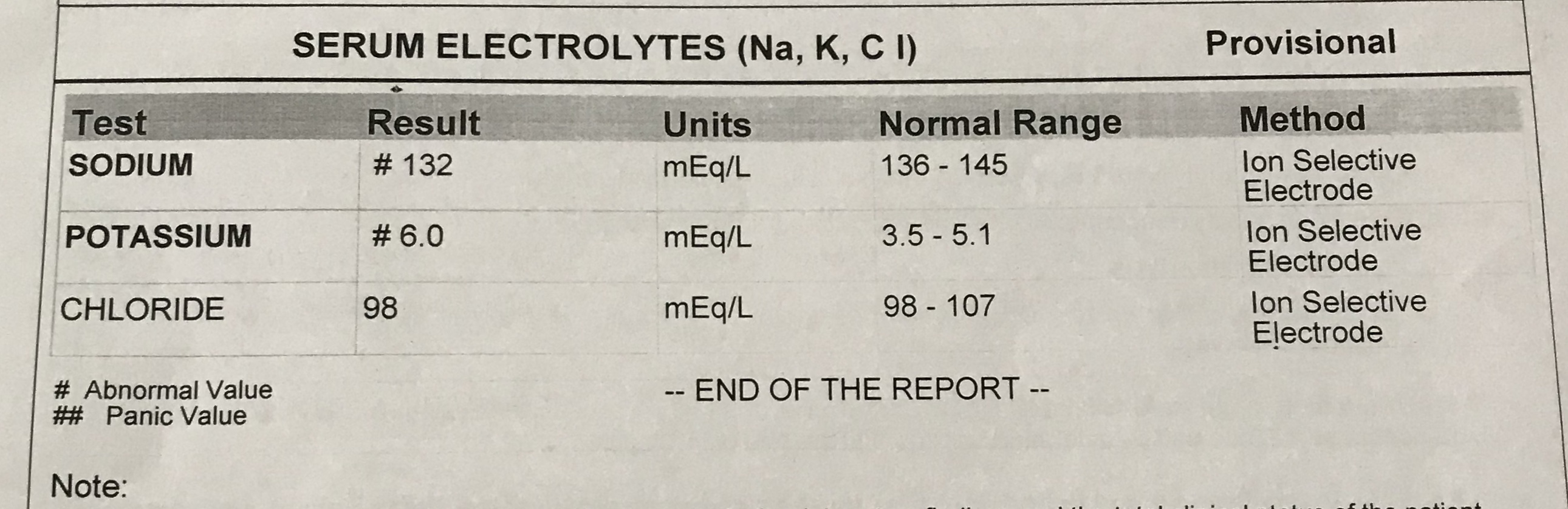
Metabolic acidosis
His Potassium continued to be on the higher end - 6
Though his urine output increased his Serum creatinine (2.4mg/dl) and blood urea (214mg/dl) have raised
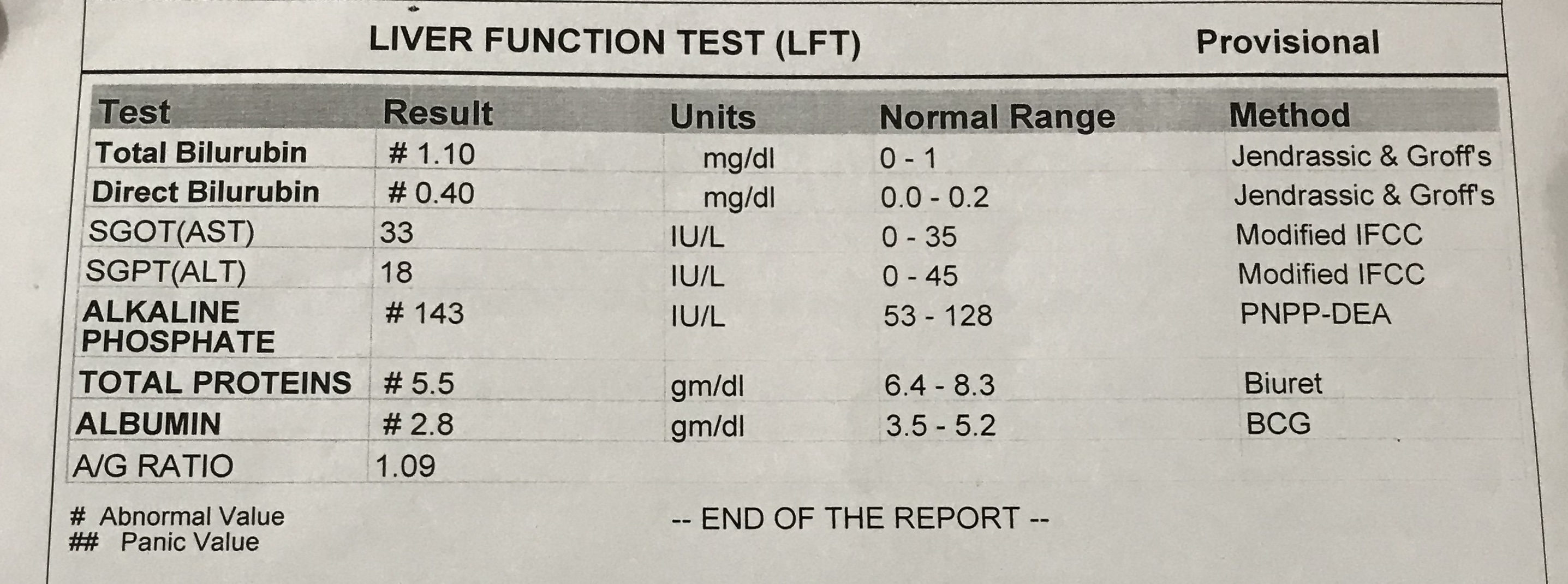
Along with total Bilirubin
TB - 1.10 ( raised)
DB - 0.40
We decided to replace his foleys catheter but were unable to pass Foleys for which Surgery opinion was taken and they adviced for Usg of pelvis and scrotal area to rule out urethral stricture which turned out to be normal , we informed the urology department as to know why we were unable to pass Foleys catheter. We decided to have look at his chest xray as the patient was complaining of cough.
Chest x ray:

Review usg abdomen:

Usg inguinoscrotal region:





Day 4:
45 year man
With ? Nephritic nephrotic syndrome with eGFR - 54
HFPeF
PAH with Mitral stenosis
HTN and DM with 15 years
Right eye cataract since 15 years
Monoplegic since 1.5 years
B/L pleural effusion with B/L infiltrates
Patient says he is able to speak better
Has resting tremors
Urine I/O - 2000/2200ml
Grbs - 184
PR - 103 Bpm
RR at 18cpm
BP- 140/90mmhg
Spo2 - 98%
Cvs - tapping apex + in MA
S1,S2+
Lungs - Inspiratory crackles in bilateral IMA,IAA
Abdomen - Diffuse tenderness
Distended
Bowel sounds +


His serum albumin was 2.8 g/dl
24 hrs urinary protein: 855mg/day ( N: <150 mg/ day)
24 hrs urine volume: 3,800 ml
24 hrs creatinine (urine) : 0.91g/day
His coagulation profile was repeated today which showed
PT to be 18 sec, INR - 1.3, aPTT - 36 SEC, BT - 2 mins 30 secs, CT - 5 mins
His urinary protein though on a higher range wasn't suggestive of nephrotic syndrome.
Nephrotic range proteinuria is usually considered to be >2g/day of protein loss.
Possible that it could be Nephritic syndrome keeping in mind the hematuria but also in advanced nephrotic syndrome it could be possible that in patients with hypoalbuminameia the protein loss might be less as there is no protein left in blood.

Comments
Post a Comment